March 18, 2025
The Big Picture
Heart disease remains the world’s leading killer, claiming nearly 18 million lives globally each year. In the U.S. alone, roughly 805,000 people have a heart attack annually—one every 40 seconds. Caristo Diagnostics is stepping into this high-stakes arena with new FDA clearance for its AI-driven plaque analysis, aiming to catch “silent” heart risk years before a major cardiac event.
- Why it matters: Caristo’s AI identifies signs of coronary inflammation and plaque that standard scans often miss. That means doctors can intervene early—potentially preventing costly hospitalizations, invasive procedures, and, ultimately, heart attacks.
Driving the News
Caristo has secured FDA 510(k) clearance for CaRi-Plaque, setting the stage for U.S. commercialization. This milestone follows a series of large-scale studies, including a 40,000-patient Lancet-published trial showing that Caristo’s inflammation-based metric (FAI-Score) can predict major cardiac events up to a decade in advance.
- State of play: The new clearance allows Caristo to officially compete with established AI cardiac imaging players like HeartFlow and Cleerly—both of which already enjoy Medicare reimbursement for similar plaque analyses.
- Catch: Caristo’s full solution (including CaRi-Heart/FAI-Score) is still pending full U.S. commercial rollout; the plaque-only component is FDA-cleared, while the inflammation-based risk scoring is currently investigational in the U.S.
Between the Lines: Market & Clinical Context
- Huge Financial Burden
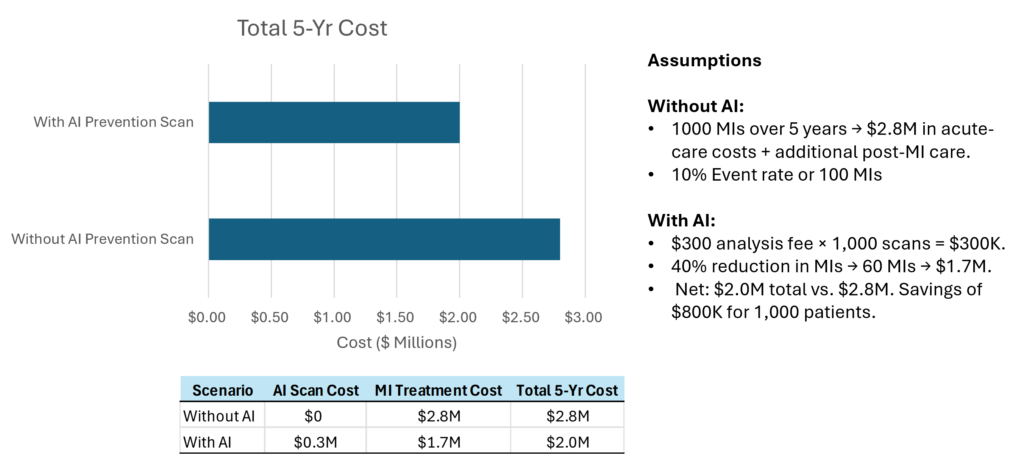
- Heart disease costs the U.S. over $100 billion a year in direct medical expenses. Each acute heart attack admission can total $25K–$30K in hospital costs alone.
- Preventing even a modest fraction of these events could yield significant ROI, especially in capitated or value-based care models.
- Reimbursement Tailwinds
- As of 2024, 4 out of 7 Medicare Administrative Contractors (MACs) already cover AI-based plaque analysis. A new Category I CPT code (75580) for AI coronary plaque (effective Jan 2026) legitimizes reimbursement, which is expected to accelerate adoption in U.S. hospitals and imaging centers.
- Private insurers often follow Medicare’s lead. By late 2025, more commercial payers are likely to cover AI-driven plaque quantification.
- Global Traction
- Europe: Early to adopt advanced cardiac CT guidelines. Caristo’s technology has CE Mark for investigational use, but broad EU adoption hinges on each country’s reimbursement and health technology assessments.
- Asia-Pacific: Poised for the fastest growth, driven by high cardiovascular disease burdens in China, India, and Japan. Local regulatory approvals (PMDA in Japan, NMPA in China) are next steps.
- LATAM & Middle East: Focused adoption in private hospital networks and “longevity clinics,” especially in Gulf states with high rates of diabetes and obesity.
Competition at a Glance
- HeartFlow: Pioneer in AI for fractional flow reserve (FFRCT), widely adopted to reduce unnecessary invasive angiograms. They recently expanded into plaque analysis.
- Cleerly: U.S.-based startup with robust traction and 510(k)-cleared AI for detailed plaque characterization. They emphasize population health and have secured major partnerships with payers.
- Artrya: Australian player focusing on vulnerable plaque. Currently awaiting FDA clearance. Primarily active in Australia, with an eye on global expansion.
- Differentiator for Caristo: Unique emphasis on coronary inflammation (FAI-Score), supported by extensive Lancet data linking inflammation to long-term risk.
Zoom In: Adoption Barriers
- Workflow Integration
- Many radiology departments worry about slow AI turnaround times or complex cloud workflows. Caristo’s “one-click” system claims a rapid return of results in DICOM/PDF format, but acceptance hinges on real-world efficiency.
- Physician Trust
- Clinicians need data and transparency. Large-scale validation (e.g., Caristo’s 40,000-patient study) is promising, but “black box” AI can face skepticism. Early adopters will likely be academic centers and tech-savvy cardiologists.
- Regulatory Patchwork
- Outside the U.S. and EU, Caristo must navigate local clearances (China, Japan, etc.). Compliance with data privacy rules—HIPAA, GDPR—is critical, especially when uploading scans to a cloud service.
- Cost & Reimbursement Gaps
- While the new CPT code is effective in 2026, near-term coverage might be patchy. Hospitals could be reluctant to pay out-of-pocket for AI analyses until full reimbursement is guaranteed.
Stakeholder Impact
- Cardiologists: Gain earlier identification of “hidden” high-risk patients—potentially revolutionizing preventive cardiology.
- Radiologists: Automated plaque quantification boosts reporting accuracy and efficiency, though some fear “AI encroachment.”
- Patients: More personalized risk assessment and potential to avoid sudden, catastrophic events. Visual AI reports can motivate lifestyle and medication adherence.
- Hospitals & Health Systems: A potential draw for proactive consumers seeking advanced heart checks. Under value-based care, fewer heart attacks = cost savings.
- Payers: Upfront AI fees, but big potential for downstream savings by preventing ER visits, stents, and bypass surgeries.
By the Numbers: Financial Outlook
- AI in Cardiology: Valued at $500M in 2024, projected to reach $4.7B+ by 2032, at ~34% CAGR.
- AI Cardiac Imaging: A substantial slice of that total, fueled by FFRCT and plaque analysis.
- U.S. Dominance: ~40–45% of the AI cardiology market stems from North America; Europe follows at ~25%. Asia-Pacific is the fastest growing, with potential to surpass Europe’s share by late decade.
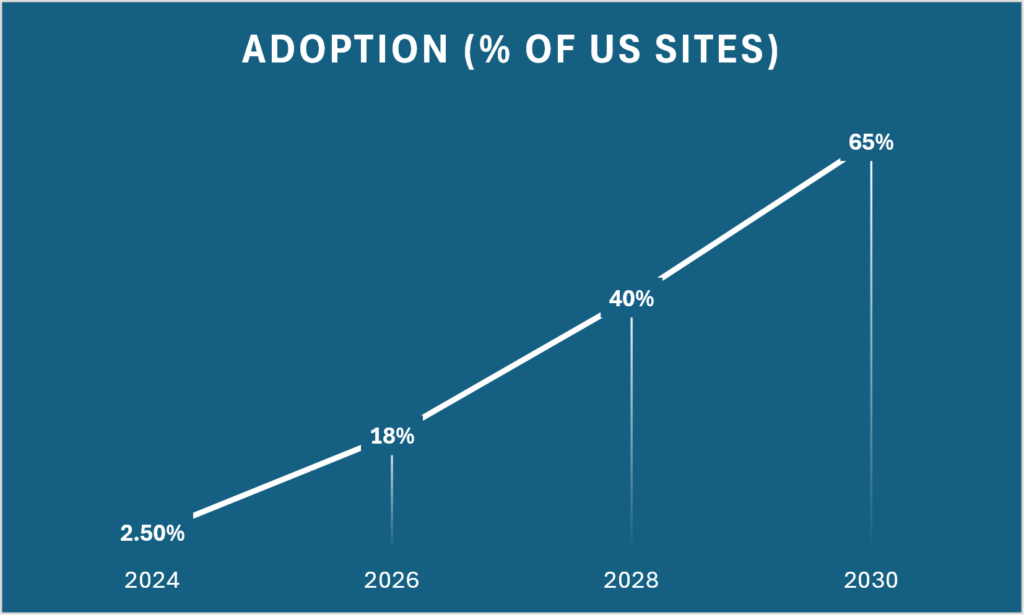
- Adoption Potential: If even 10% of ~18 million annual U.S. cardiac tests switch to AI-based CCTA, that’s 1.8 million scans/year—likely a multi-hundred-million-dollar opportunity.
Our Thought Bubble
Caristo’s FDA clearance checks a crucial box for U.S. entry, placing it in direct competition with the likes of HeartFlow and Cleerly. However, Caristo’s unique inflammation-based detection could give it a powerful edge—especially in preventive cardiology, a space not yet dominated by legacy AI players.
- What to watch:
- Medicare decisions in 2025–26. Positive local coverage determinations will be the tipping point for hospital adoption.
- Guideline endorsements from major societies like ACC/AHA. If guidelines embrace AI-based plaque/inflammation as standard of care, that supercharges adoption.
- Big OEM partnerships. Deals with CT manufacturers (e.g., Siemens, GE) would accelerate global scale and build a user-friendly workflow.
What’s Next
With Caristo gearing up for U.S. deployments (and eventual FDA clearance for its full inflammation-scoring product), watch for:
- Health systems rolling out pilot “AI-CT” programs to catch hidden cardiac risks.
- Evolving reimbursement that broadens coverage beyond symptomatic patients, opening the door for proactive screening in asymptomatic adults.
- Head-to-head clinical data pitting Caristo’s inflammation-based approach against other AI plaque platforms to see which best predicts—and prevents—major adverse cardiac events.
Bottom line: Caristo’s FDA greenlight signals that AI-driven heart attack prevention is moving from concept to clinic. As real-world evidence accumulates, early intervention—powered by advanced imaging—could reshape cardiac care worldwide, saving lives and dollars in a healthcare system that urgently needs both.